By Maria Rylott-Byrd, BA (Hons), CIDESCO, CIBTAC, AET, Madame Chair, I.A.C.
The International Association for Applied Corneotherapy (I.A.C.) defines Corneotherapy as ‘a remedial skin treatment methodology with its core principle being the repair and maintenance of the skin barrier defence systems’.[1]
It is a systematic, evidence-based process that supports the skin’s own defence mechanisms and promotes long-term, sustainable health rather than short-term gratification.
Its lineage can be traced back to Professor Albert M. Kligman and his peers who, through their research, established that the Stratum Corneum (SC) had ‘become very much alive’; [2] a discovery which redefined the way we approach caring for skin. Indeed, it marked a shift from prioritising visible symptoms towards restoring physiological function.
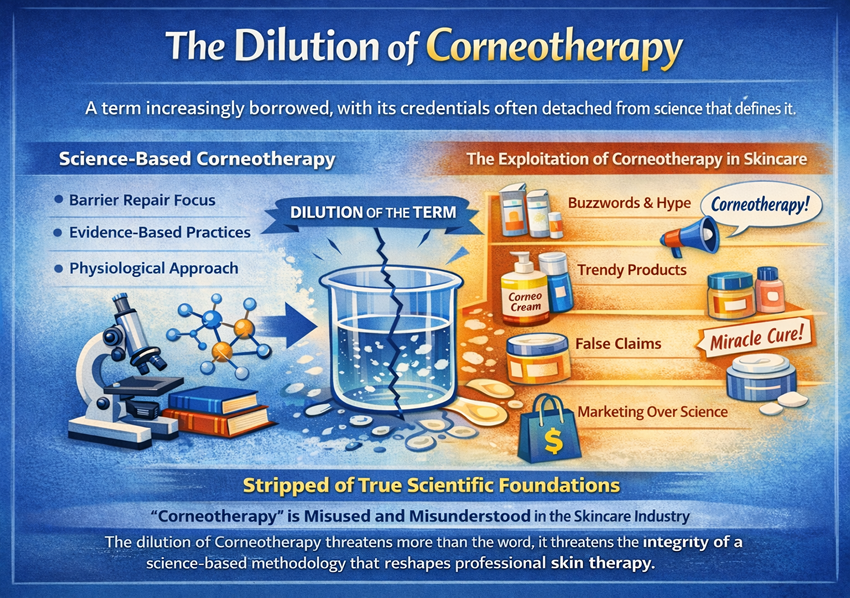
Yet, despite its scientific foundation, Corneotherapy is a term being increasingly borrowed, with its credentials very often detached from the science that defines it.
Not a trend to be exploited
It’s not uncommon to see brands describing their products as corneotherapeutic simply because they are skin barrier friendly. Yet, unless those formulations meet the precise criteria for corneotherapeutic formulation, they fail to qualify as such.
A product may of course be inspired by Corneotherapy, but under no circumstances does this automatically constitute a corneotherapeutic formulation.
A further concern is the rise of practitioners offering what purports to be corneotherapeutic practices, whilst actively contradicting the very principles that make it corneotherapeutic in the first place. It must be understood that Corneotherapy is not a trend to be exploited, it’s an applied science that must be preserved and respected.
The industry is also now witnessing reinventions of Corneotherapy, with practitioners and marketeers claiming their own ‘hybrid’ methodologies. Let’s be clear, Corneotherapy is not open to interpretation. You either practise it, or you do not. To blend Corneotherapy with incompatible modalities or incompatible topical formulations to suit a different narrative severs it from its corneobiological foundations, rendering it non-corneotherapeutic.
In reality, to practice only parts of Corneotherapy is to practise something else entirely.
Corneotherapy’s power lies in its precision. The moment those principles are ignored, the methodology loses efficacy and the term loses integrity.
Inappropriate Practice
Thanks to Kligman et al, we know the SC is far from a passive layer of dead cells. It is, in fact, an active, dynamic structure essential to skin health, responsible for, but not limited to, “regulating epidermal water content…mitigating exogenous oxidants…preventing or limiting cutaneous infection...responding via innate immune mechanisms to “cutaneous invaders” of many origins…and protecting its neighboring cutaneous cells and structures that lie beneath from damaging effects of ultraviolet radiation”.[3]
Barrier science, particularly the work of Elias and Feingold (2012), showed that ceramides, cholesterol and free fatty acids must exist in a 1:1:1 molar ratio to maintain barrier integrity.
Disrupt this ratio and you’ll increase trans-epidermal water loss (TEWL), stimulate immune responses and trigger inflammation.[4]
There also seems to be a misconception that Corneotherapy is too gentle to be effective, but by nurturing the skin’s physiology to achieve homeostasis, the skin itself can progressively mitigate its own issues.[5] Creating this balance requires a deep understanding of how the skin functions and the role of credible corneotherapists is to support, not force, these innate processes.
Inappropriate practice of Corneotherapy only serves to mislead consumers and confuses practitioners entering the space. It suggests that avoiding certain ingredients or offering ‘mild’ facials qualifies as Corneotherapy, when it unequivocally does not.
The I.A.C. strives for global standards to protect Corneotherapy and prevent ambiguity,in order to ensure consistency and integrity. However, all ethical stakeholders have a duty of care to uphold True Corneotherapy, as the clinical methodology it is. It must not be watered down for commercial gain.
To preserve legitimacy, brands and educators have a moral responsibility to use the term only when it aligns fully with corneotherapeutic principles and standards. Practitioners must remain critical thinkers, seeking credible education, understanding skin biochemistry, whilst resisting the perpetual industry distractions.
Corneotherapy does not need to be reinvented, it needs protecting, from misuse,mislabelling and misinterpretation. It stands firmly and proudly on decades of dermatological and corneobiological evidence.
Conclusion
The dilution of Corneotherapy threatens more than the word, it threatens the integrity of a science-based methodology that reshapes professional skin therapy.
There should be no hybrids, no half-in-half-out practitioners and no grey areas! Corneotherapy is and will always remain a discipline grounded in skin science, ethics and integrity. When we uphold this, we protect not just a methodology, but the results it delivers, the clients it serves and the credibility of our profession.
References used in this article:
1. International Association for Applied Corneotherapy. What is Corneotherapy (2010) www.corneotherapy.org
2. Kligman, A.M. (2011), Corneobiology and Corneotherapy – a final chapter.
International Journal of Cosmetic Science, 33: 197-209.
https://doi.org/10.1111/j.1468-2494.2011.00644.x
3. Del Rosso JQ, Levin J. The clinical relevance of maintaining the functional integrity of the stratum corneum in both healthy and disease-affected skin. J Clin
Aesthet Dermatol. 2011 Sep;4(9):22-42.
https://pmc.ncbi.nlm.nih.gov/articles/PMC3175800/
4. Elias, P.M. & Feingold, K.R. (2012). Skin Barrier: Chemistry, Physiology and Pathophysiology. CRC Press.
5. Del Rosso JQ, Kircik L. Skin 101: Understanding the Fundamentals of Skin Barrier Physiology - Why is This Important for Clinicians? J Clin Aesthet Dermatol. 2025
Feb;18(2):7-15. https://pmc.ncbi.nlm.nih.gov/articles/PMC11896616/